
Global Information Hub on Integrated Medicine.2017.pg 1-13.
Terence Tan Yew Chin1, Siti Habsah Sheikh Zahari1, Teh Bee Ping1, Siti Khairul Bariyyah Akhiar1, Nurul Ashkin Ismail1, Syazlina Khairuddin1, Raja Nazatul Izni1, Norazila Zulkarnain1
1 Herbal Medicine Research Centre (HMRC), Institute for Medical Research, Malaysia
Contact address
Terence Tan Yew Chin, Herbal Medicine Research Centre (HMRC), Institute for Medical Research, Jalan Pahang, 50588 Kuala Lumpur Malaysia.
[email protected] ; [email protected]
Editorial group
GlobinMed, Traditional and Complementary Medicine Division
Publication status and date: Published in JANUARY, 2017.
Citation
Terence TYC, Siti HSZ, Teh BP, Siti KBA, Ashikin I, Syazlina K, Nazatul RI, Norazila Z. Homeopathy for the treatment of headache disorders. Global Information Hub on Integrated Medicine 2017, Issue 1. Art. No.: CD003803. DOI: 10.1002/14651858.CD003803. Copyright © 2017 Published by GlobinMed.
ABSTRACT
Background
Forty-seven percent of the adult population (majority aged 18-65 years) is estimated to suffer from headache disorders which can be divided into primary and secondary headaches in the year 2011 although it has been underestimated, under-recognised and under-treated globally. Homeopathy is a 200-year-old health care system categorised under complementary treatment with over 3000 available remedies.
Objective
To conduct a review on peer-reviewed and published trials on the effectiveness of homeopathic medications used in treating headache disorders as determined by the International Headache Society.
Search Strategy
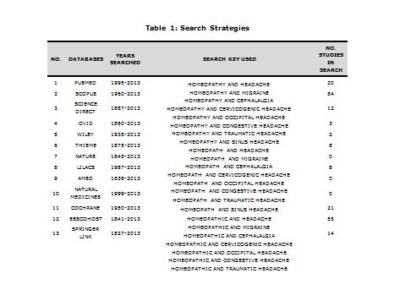
The trials were identified from a search of the Pubmed, The Cochrane Library, Scopus, ScienceDirect, Springer Link, Ovid, Wiley, Thieme, Nature, LILACS, EbscoHost, AMED and Natural Medicines comprehensive database sources in June 2013 using the terms homeopathy*, homeopath*, migraine”, headache” and others .
Selection Criteria
Only randomised control trials were included.
Data Collection and Analysis
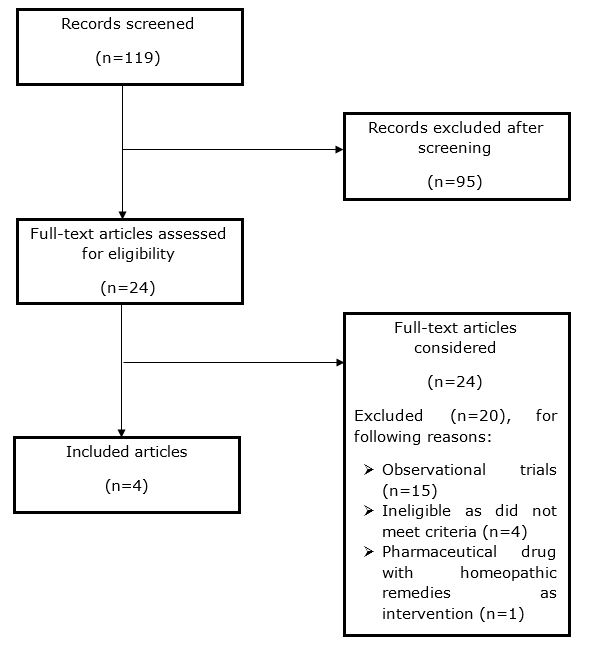
The database search resulted in 119 abstracts being identified. After examining the abstract, the full paper was obtained and independently assessed for inclusion by the principle author and co-authors depending on the 13 databases that were equally distributed among four groups (two individuals in each group).
Main Results
A total of four RCTs with 322 participants met the inclusion criteria. Out of four RCTs, two papers were focused on primary headache disorders and the remaining two studies involved patients with secondary headache disorders. The studies involved a sample size of 63 to 98 subjects ranging from four months to one year study duration. Interventions in four studies were individualised homeopathic prescriptions. From the review conducted, we found that homeopathy was superior to placebo in one randomised clinical trial whereas in three other trials were equal or less effective than placebo in treating headaches. Adverse effects were also reported in two of the studies using homeopathic treatment. Therefore, further investigations should be conducted with proper methodology on the therapeutic effectiveness of homeopathic treatment for headache disorders.
KEYWORDS- Homeopathy, homeopath, headache, migraine, cephalalgia
INTRODUCTION
Forty-seven percent of the adult population (majority aged 18-65 years) is estimated to suffer from headache disorders in the year 2011 although it has been underestimated, under-recognised and under-treated globally [1].
Headache disorders can be divided into primary headaches consisting of tension-type headaches and migraines while secondary headaches can consist of fasting headaches, sinus headaches, traumatic headaches and non-vascular intracranial disease [2].
The prevalence rates, using a population-based survey in Japan that met the International Headache Society criteria were 8.4% for migraine and 22.4% for tension-type headaches [3]. The one-year prevalence of migraine in the United States is 13% with the highest occurrence between 25 to 55 years of age [4].
In a study conducted in Baltimore, USA, the prevalence rates based on gender in having frequent headaches were 5% in women and 2.8% in men. The two most common headaches identified were chronic tension-type headache and transformed/chronic migraine [5]. Another study which estimated the one-year period of episodic tension-type headache showed prevalence as high as 38.3% of the population in Baltimore, USA whereby the headache peaked in the 30 to 39 year old group [6]. The Centre for Disease Control reported that the prevalence of migraine in US increased from 25.8 per 1000 persons to 41.0 per 1000 persons from 1980 to 1989 [7].
The homeopathy health care system was founded by Samuel Hahnemann 200 years ago [8]. The clinical practice of Homeopathic treatment is based on case-by-case, or individualised method. In selecting a course of care, homeopath practitioners often use a method called “classical” or “constitutional” prescription, where a specific homeopathic remedy is matched to the specific aspects of the patient’s complaints. Through this method, the specific selection of the remedies depends not only on the symptoms and the disease itself, but also on the nature, temperament, disposition, constitution, vitality and lifestyle of the patient. This approach is thought to result in high patient satisfaction, as well as improved outcomes [9]. There are over 3,000 available remedies used in homeopathy treatment and the most commonly available strength is 30C potency, which is highly diluted [10].
During the past decade, the interest in complementary and alternative medicine (CAM) has increased and the attitude of the general public towards it is mainly positive. The prevalence of complementary and alternative medicine (CAM) use in the UK showed that homeopathy was the second most popular and is widely used in Western European countries including France, Germany and the Netherlands. Homeopathy is also popular in the Indian subcontinent and Latin America and recently there has been rapid growth of usage in the USA [11].
In a study conducted in Norway on the characteristics of people visiting homeopaths in a total adult population, it showed that a person consulting a homeopath was most strongly associated with being female and having a lower perceived global health. There was also a trend for increased likelihood of visits to homeopaths for those 60 years and over, social welfare recipients, having a chronic complaint and a HADS-T score of 20 or higher [12].
In Brazil, prevalence of the use of homeopathy was at 2.4%. The factors associated with its use were female gender, schooling and income. The main reason that led to homeopathy treatment was that the patients believed “conventional treatment did not have any effect” on them. For 70.2% of the users, the cost of the treatment was considered reasonable or cheap and about 73% were satisfied or very satisfied with the treatment received through homeopathy [13]. A study showed that 3.2% of total patients sought the homeopathic physician for treatment of headaches and migraines [14].
The extensive use of homeopathy, together with positive interest in homeopathy as a treatment for headaches suggested that a review of the evidence of its effectiveness would be valuable.
In this study, we will conduct a review on peer-reviewed and published trials on the effectiveness of homeopathic medications used in treating migraines or other headache disorders as determined by the International Headache Society.
OBJECTIVES
- To evaluate the effectiveness of homeopathic medications used in treating headache disorders such as the intensity, frequency and duration of the attacks.
- To evaluate the appropriateness of the duration of homeopathic treatment for headache disorders.
METHODS
Data Searching
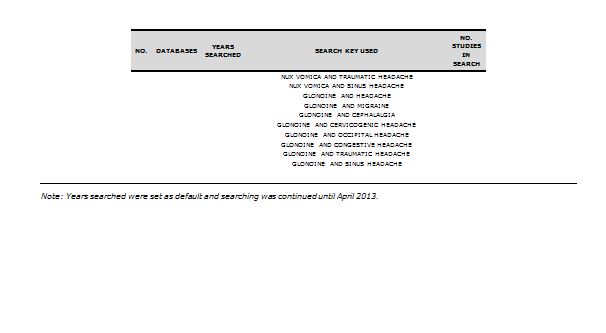
Thirteen databases were searched with 64 search keys (as shown in Table 1) to identify related published articles. Studies were further identified by searching the citations and list of references in relevant review and critique articles. Initially, studies with English and other languages articles were included. Seven authors were involved in the extensive literature search by dividing the list of databases. At least two authors were responsible in one list of divided databases by performing literature search independently and then cross-checking their search. Years searched were set as default and searching was continued until April 2013. The literature search resulted in the identification of 119 published articles. Results of the search are showed in Figure 1.
Selection of Samples
Adults aged above 18 years old with headache disorders were eligible for selection. Classification criteria for primary and secondary headaches are as defined in The International Classification of Headache Disorders, 2nd Edition (ICHD-II)[15]. Studies involving patients with primary and secondary headaches were included.
Selection of Intervention
Only individualised or randomised homeopathy treatment (with any type of form and dosage) were considered. The duration of therapy was to be from one month to one year without taking the follow-up period into account.
Selection of Comparison
From the randomised controlled trials (RCTs), only homeopathy treatment compared with placebo was chosen.
Selection of Outcomes
Studies reporting clinical outcomes related to headache disorders were eligible such as relief of the headache disorders including reduction of recurrence frequency, reduction of duration of each attacks, reduction of pain severity and/or decreased pain intensity.
Selection of Study Model
Only RCTs were included.
Data Extraction
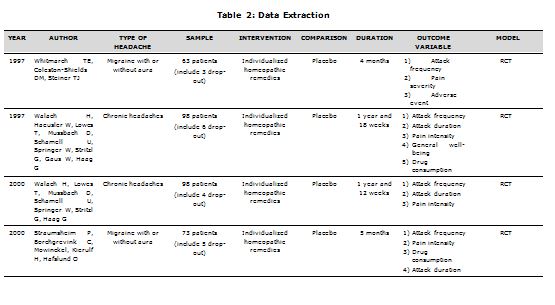
All searched articles were read in full text. Each article was screened based on selected samples (or participants), intervention, comparison, outcomes, and study model (or study design). Only English articles were evaluated and extracted. This screening resulted in the identification of 24 related full text articles but only four RCTs full texts which met our selection criteria. At least two authors independently extracted the above four articles into a standardised table, as described in Table 2, to minimise biasness.
Limitations
Review and critique articles, non-published articles, and books were excluded from this review since it does not meet the criteria set for this review which is to focus on study models with higher evidence levels. This review article uses no methodological quality assessment on the extracted studies because it is not supported by empirical evidence [16][17]. It is also difficult to justify the weights assigned for different items in the scale used for calculating a summary score. In addition, use of scales as validity assessment has been shown to be inappropriate [18] and less likely to be transparent to readers of the review. Hence, it is preferable to use simple approaches for assessing validity that can be fully reported (i.e. how each trial was rated on each criterion). There was no year restriction on the RCT articles included.
RESULTS
A total of four RCTs were included in this review [6][17][18][19]]. The appraisal of each study is presented in Table 2.
Out of the total four RCTs, two papers were focused on primary headache disorders [16][17]. The remaining two studies involved patients with secondary headache disorders [18][19]. The studies involved a sample size ranging from 63 to 98 subjects. Two studies had a four to six month study duration [16][17] while two studies had a longer duration of more than six months to one year because these articles involved a one year follow-up period [18][19]. Interventions in the four studies were individualised homeopathic prescriptions [16][17][18][19].
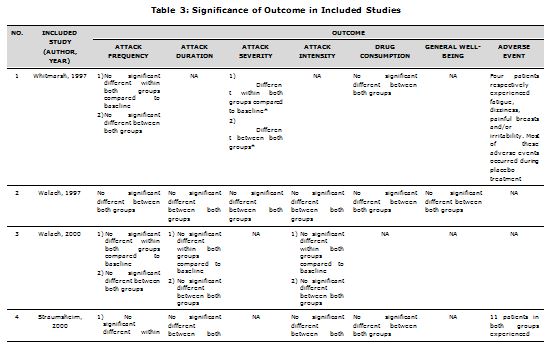
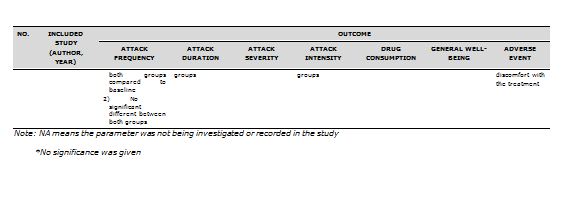
The outcome variables measured from the homeopathic intervention in the studies were: frequency, intensity, severity, duration, general well-being, adverse event and/or level of medication necessary for attacks. All three RCTs showed no significant difference in homeopathic remedy group compared to either baseline or placebo, as shown in Table 3 [16][17][18][19], except for one in which no further detail on significance was mentioned for the parameter measured [19].
In terms of quality assessment of the chosen studies, dropouts were partially described and accounted for in all four clinical trials. Inclusion and exclusion criteria were also clearly mentioned in all four clinical trials although two out of four studies did not specifically mention the age range [18][19]. Partially adequate follow-up intervention after post-treatment was observed in two studies [17][18] while the remaining two studies had no follow-up intervention [16][18]. Three studies had comparison groups such as placebo or existing efficacious or commonly practiced treatment option(s) [16][17][19] while the remaining one study did not [18]. Confidence intervals (CI) were included in two studies [16][17] in the value of 95% where all p-values of 0.05 or less were considered as significant. Two studies did not state their confidence intervals [18][19]. Two studies reported adverse effects during the homeopathic treatment such as discomfort, fatigue, dizziness, painful breasts and irritability [16][17].
DISCUSSION
The effectiveness of homeopathy from the included RCTs
The effectiveness of homeopathy treatment for headache disorders can be determined by investigating the homeopathy treatment compared to placebo. From the review conducted on the selected studies, homeopathy was equal or less effective than placebo in treating headaches [16][17][18][19]. There were two studies that reported homeopathy treatment with adverse effects [16][17]. Out of the four RCTs, two studies had a four to six month study duration [16][17] while two studies had a longer duration of more than six months to one year because these articles also involved a one year follow-up period [18][19].
From the results obtained above, it is clear that the main issue is similar to earlier studies on whether homeopathy is effective or acts as a placebo. A meta-analysis indicated that there is insufficient evidence for homeopathy to be effective for any single clinical condition [20]. Although efforts have been made by conducting controlled clinical studies to make the study peer-reviewed and scientific evidence based, there are still limitations and the quality of the study has to be considered through validity methods for the proper determination of homeopathy effectiveness. However, it cannot be discarded that homeopathy has shown a positive response in patients with chronic illnesses as a clinical audit reported that 64% of patients with headaches showed an improvement after homeopathic treatment using the Glasgow Homeopathic Hospital Outcome Scale [21]. There are also suggestions that homeopathy can be catered to the paediatric population instead [22].
Study limitations in the included RCTs
There are many factors that can affect the validity of homeopathy effectiveness. First would be poor description of hypotheses and objectives of the studies due to inadequate statistical evaluation, small sample size and soft primary endpoints which do not require subjective assessments from investigators as well as inconsistent blinding methods of subjects involved in the study [23][24]. However, a study debunked the theory by showing that a small sample size has a significant difference in quality, favourable to homeopathy [25]. Apart from that, the outcomes of the studies were highly variable [26] which led to questionable methodology such as lack of evidence to show that homeopathy was highly effective for a certain condition and require better trials to be conducted [20]. There is also a tendency for selection biasness if there are too few literatures to assess and this makes the interpretation difficult [20][27].
By focusing on each particular article, we found that the article by Straumsheim and colleagues [17] consisted of a partial explanation of the primary outcomes biasness and statistical non-significant results [23]. Other limitations are unreliable ratings by the physicians on the attack frequency which contradicted the findings from patient’s evaluation and diaries, the homeopathic treatment was not isolated from other interventions (such as the use of ergotamine), not blinded enough as the homeopathic researcher interviewed the patients prior to the start of treatment, no standard homeopathic prescription and the comparison level in the baseline group was set too high, i.e. 18 patients in baseline group had more than 6 attacks.
In Whitmarsh and colleagues’ article [16], the baseline differences of primary endpoint affected the interpretation of the article which could have been solved [23] using stratification. Furthermore, differentiation of scope occurs when non-standardised therapy was determined by the individual therapist [16][23]. Other limitations are limited follow-up period (should be longer), differences within the baseline itself, cross-over and therapies involved were not standardised as they were dependent on the therapist’s judgments.
In both articles by Walach with different colleagues’ [18][19], the use of analgesics by the homeopathic group was more than the placebo group due to long periods of aggravation. This will indirectly affect the outcome variables of the study since the pattern of analgesic use was not mentioned. Another factor not considered would be the period of long-standing headache the patients were suffering. The selection of homeopathic treatment was affected due to the years of persistent headache suffered by the patients who may not be cured by first homeopathic medicine [28][29].
Improvement of quality of study
A majority of these studies should be applauded for making an effort to come up with a suitable experimental design to exhibit homeopathy effectiveness in treating headaches but certain issues have to be resolved before a legitimate interpretation can be made [28].
The most important issue would be identifying a research model with both high relevance to homeopathic practice and rigorous research protocols detailing the trial process such as patient response, prescriber’s selection of homeopathic remedy and follow-up feedback [26][30]. By performing a pilot study, a large sample size can be monitored and evaluated with ease [31]]. The proper method before conducting the study would be to develop a protocol as recommended called the Consolidated Standards of Reporting Trials (CONSORT) which contains adequate trial reporting such as a checklist and flow diagram to facilitate the critical appraisal and interpretation of RCTs [23].
A longer study period should be conducted for long-standing headaches, by at least two years. If this is not possible, it is recommended that the selection of patients for the study involve those suffering from short duration of headaches. No analgesic drugs should be taken by the patient during the aggravation period for a clearer picture of the outcome. Each prescriber enrolled in the study should pursue the patient’s case separately in order to determine the choice of homeopathic medication accurately since it is selected individually before comparison [29]. For the choice of homeopathic treatment, standardisation of remedy should be identified differentiating the features of the symptoms [32]. If this is not possible due to the variance of remedy usage, similimum is recommended [33].
The quality of each study conducted should be assessed by performing two quality scores. The first will evaluate the random allocation, double-blinding, and the reporting of withdrawals whilst the second will cover the adequacy of concealment, the handling of withdrawals, baseline group comparability, and the adequacy of inferential statistics. The application for each trial must be done by two independent reviewers, with further discussion for contradictory results. Inter-observer reliability before discussion was checked with the intraclass correlation coefficient for both validity scores [20].The precision of the study should also be conducted using the pseudo replication method [34].
CONCLUSION
In conclusion, a majority of the studies selected for review had limitations or flaws in the design of their study. There was also a small quantity of randomised trial studies to review which makes it difficult to support or disprove the use of homeopathy for treatment of headache disorders. It is possible that further studies do exist in languages other than English, especially considering that homeopathy is so widely practiced in mainland Europe.
From the review conducted, we found that homeopathy was superior to placebo in one randomised clinical trials whereas in three others, were equal or less effective than placebo in treating headaches. There were also two studies where homeopathy treatment were reported to have adverse effects. Thus, further investigation should be conducted with proper methodology on the therapeutic effectiveness of homeopathic treatment for headache disorders.
ACKNOWLEDGEMENT
The authors would like thank the Director General of MOH for his permission to publish this review paper. Also, the authors would like to acknowledge the review team members for their valuable efforts in completing this review successfully.
APPENDIX
REFERENCES
- Fact sheet: Headache disorders World Health Organization; 2012 October [cited 2013 July 13]. Available from: http://www.who.int/mediacentre/factsheets/fs277/en/.
- Rasmussen BK, Jensen R, Schroll M, Olesen J. Epidemiology of headache in a general population–a prevalence study. J Clin Epidemiol. 1991;44(11):1147-57.
- Sakai F, Igarashi H. Prevalence of migraine in japan: A nationwide survey. Cephalalgia. 1997;17(1):15-22.
- Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the united states: Data from the american migraine study ii. Headache. 2001;41(7):646-57.
- Scher AI, Stewart WF, Liberman J, Lipton RB. Prevalence of frequent headache in a population sample. Headache. 1998;38(7):497-506.
- Schwartz BS, Stewart WF, Simon D, Lipton RB. Epidemiology of tension-type headache. JAMA. 1998;279(5):381-3.
- Chai NC, Rosenberg JD, Lee Peterlin B. The epidemiology and comorbidities of migraine and tension-type headache. Tech Reg Anesth Pain Manag. 2012;16(1):4-13.
- S H. Organon of medicine. 5th ed ed. New Dehli, India: B Jain Publishers; 1994.
- Eisenberg DM, Kessler RC, Van Rompay MI, Kaptchuk TJ, Wilkey SA, Appel S, et al. Perceptions about complementary therapies relative to conventional therapies among adults who use both: Results from a national survey. Ann Intern Med. 2001;135(5):344-51.
- J. C. A dictionary of practical materia medica. New Dehli, India: B Jain Publishers; 1994.
- Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, et al. Trends in alternative medicine use in the united states, 1990-1997: Results of a follow-up national survey. JAMA. 1998;280(18):1569-75.
- Løhre A, Rise MB, Steinsbekk A. Characteristics of visitors to practitioners of homeopathy in a large adult norwegian population (the hunt 3 study). Homeopathy. 2012;101(3):175-81.
- Rodrigues-Neto JF, Figueiredo MF, Faria AA. Prevalence of the use of homeopathy by the population of montes claros, minas gerais, brazil. Sao Paulo Med J. 2009;127(6):329-34.
- Jacobs J, Chapman EH, Crothers D. Patient characteristics and practice patterns of physicians using homeopathy. Arch Fam Med. 1998;7(6):537-40.
- Headache Classification Subcomittee of the International Headache Society. The international classification of headache disorder. 2nd ed. Oxford, UK: Blackwell publishing; 2004.
- Whitmarsh TE, Coleston-Shields DM, Steiner TJ. Double-blind randomized placebo-controlled study of homoeopathic prophylaxis of migraine. Cephalalgia. 1997;17(5):600-4.
- Straumsheim P, Borchgrevink C, Mowinckel P, Kierulf H, Hafslund O. Homeopathic treatment of migraine: A double blind, placebo controlled trial of 68 patients. Br Homeopath J. 2000;89(1):4-7.
- Walach H, Lowes T, Mussbach D, Schamell U, Springer W, Stritzl G, et al. The long-term effects of homeopathic treatment of chronic headaches: 1 year follow up. Cephalalgia. 2000;20(9):835-7.
- Walach H, Haeusler W, Lowes T, Mussbach D, Schamell U, Springer W, et al. Classical homeopathic treatment of chronic headaches. Cephalalgia. 1997;17(2):119-26.
- Linde K, Clausius N, Ramirez G, Melchart D, Eitel F, Hedges LV, et al. Are the clinical effects of homeopathy placebo effects? A meta-analysis of placebo-controlled trials. Lancet. 1997;350(9081):834-43.
- Sevar R. Audit of outcome in 455 consecutive patients treated with homeopathic medicines. Homeopathy. 2005;94(4):215-21.
- Danno K, Colas A, Masson JL, Bordet MF. Homeopathic treatment of migraine in children: Results of a prospective, multicenter, observational study. J Altern Complement Med. 2013;19(2):119-23.
- Owen JM, Green BN. Homeopathic treatment of headaches: A systematic review of the literature. J Chiropr Med. 2004;3(2):45-52.
- Ernst E. Homeopathic prophylaxis of headaches and migraine? A systematic review. J Pain Symptom Manage. 1999;18(5):353-7.
- ALB Rutten, Stolper C. The 2005 meta-analysis of homeopathy: The importance of post-publication data. Homeopathy 2008;97:169–77.
- Riley D, Fischer M, Singh B, Haidvogl M, Heger M. Homeopathy and conventional medicine: An outcomes study comparing effectiveness in a primary care setting. J Altern Complement Med. 2001;7(2):149-59.
- Whitmarsh T. Long-term follow-up after homeopathic treatment of chronic headache. Do not generalise from such a special case2001. 61-2 p.
- Vithoulkas G. Homeopathic treatment of chronic headache: A critique. Homeopathy. 2002;91(1):32-4.
- Muscari-Tomaioli G, Allegri F, Miali E, Pomposelli R, Tubia P, Targhetta A, et al. Observational study of quality of life in patients with headache, receiving homeopathic treatment. Homeopathy. 2001;90(4):189-97.
- Gaus W, Hogel J. Studies on the efficacy of unconventional therapies. Problems and designs. Arzneimittelforschung. 1995;45(1):88-92.
- Medhurst R. Homoeopathy and its role in the management of headaches. J Aust Tradit Med Soc. 2011;Volume 17 (Issue 2):24-5.
- Cooper DJ. Migraine. A homoeopathic aproach. Br Homeopath J. 1984;73(1):1-10.
- Ernst E. A systematic review of systematic reviews of homeopathy. Br J Clin Pharmacol. 2002;54(6):577-82.