2.1 SPORTS PERFORMANCE AND CHIROPRACTIC
A 1991 study by Lauro, et al investigated chiropractic effects on athletic ability. The study involved fifty athletes and they were tested on 11 different parameters. The study subjects were divided into two groups. Group one underwent chiropractic adjustments and group two were the control group. The eleven tests measured athletic abilities such as agility, balance, power and reaction time. At 6 weeks follow-up, group two showed minor improvement in eight tests. However group one (chiropractic group) improved notably in all the tests. For example, in a test measuring the speed of reaction of the hand to a visual stimulus, group two showed less than a 1% response while group one showed a more than an 18% response. At further follow-up at 12 weeks, group one showed more than 30% improvement [1].
2.1.2 WINTER OLYMPICS AND CHIROPRACTIC
Recent events have seen Chiropractic involvement in the Sporting Arena to a greater extent than ever before. In the Quarterly World Report from the World Federation of Chiropractic (WFC) the President, Dr Stathis Papadopoulos reported that Chiropractic services were included in the host medical team for the Vancouver 2010 Winter Olympics and Paralympics. There were 22 chiropractors on the host team, with a further four on the Canadian and five on the American teams. [2]:
2.1.3 SWEDISH STUDY
A Swedish study completed in 1999, reported improved non-muskuloskeletal symptoms after chiropractic spinal manipulative therapy. The Senior researcher, Dr CharlotteLeboeuf-Yde, DC, PhD of the Medical Research Unit, Amtsrådhuset, Torvet, Denmark, previously Nordic Institute for Chiropractic and Clinical Biomechanics, Odense, Denmark,and her fellows, submitted their findings as recorded in the Journal of Manipulative and Physiological Therapeutics. [3]
The objective of the study was to investigate for positive changes in non-musculoskeletal symptoms after chiropractic adjustment. The study was conducted in private practices in Sweden using a standardized recall interview. The patients needed to have undergone a chiropractic treatment and were asked to report any improvement in non-musculoskeletal symptoms following the treatment.
About one-quarter of the patients reported a response from the treatment. Most often cited were “easier to breath”, improved digestive function, improved vision and improved circulation. See figure below:
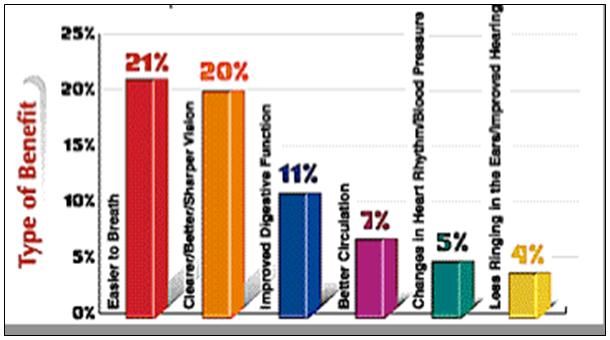
Figure 1: Additional benefits of chiropractic care
(Figure 1 adapted from Cascade Wellness Clinic. Benefit of chiropractic and massage.1997-2010. URL:http://www.cascadewellnessclinic.com/benefits.shtml) [3]
2.2 SAFETY
Chiropractic care in general is safe for people of all ages when employed skillfully and appropriately. Unfortunately, some critics of chiropractic have endeavoured to mislead the public into thinking chiropractic treatment is dangerous but nothing could be further from the truth. Chiropractic care is among the safest treatments used within the health care field today.
Previously mentioned chiropractic studies have clearly demonstrated this fact. Vis;
- The Manga Report [4]
- The Agency On Health Care Policy And Research Study [5], [6]
- The report of the Commission of Inquiry: New Zealand [7]
- The Osteopathy, Chiropractic and Naturopathy Committee: Victoria Australia [8]
2.2.1 THE MANGA REPORT: CANADA
The Manga report identified that certain medical treatments are at least as safe as chiropractic. They also found that many medical treatments could be considered unsafe and create iatrogenic complications for patients. The Manga report noted that there was no clinical or case-control studies that show chiropractic spinal manipulation was unsafe as atreatment for lower-back pain. [4]
2.2.2 1994, THE AGENCY ON HEALTH CARE POLICY AND RESEARCH STUDY: USA
The AHCPR study of 1994 found that that it was rare for serious complications to arise from lumbar spinal manipulation. Conservative treatment should be used before surgery for back pain and that includes the use of spinal manipulation. For acute lower back pain many Prescription drugs such as oral steroids are not recommended [9].
2.2.3 THE REPORT OF THE COMMISSION OF INQUIRY: NEW ZEALAND
The New Zealand Commission of Inquiry identified many pertinent points about the safety of Chiropractors and spinal manipulation. They noted that chiropractors were the only health practitioners that were properly educated and trained to perform spinal manipulation. They also found that the spinal diagnosis and therapy as performed by chiropractors was sophisticated and refined. Thus they concluded that spinal manipulation by a registered chiropractor is safe. [10]
2.2.4 THE OSTEOPATHY, CHIROPRACTIC AND NATUROPATHY COMMITTEE: VICTORIA AUSTRALIA
This All-Party Parliamentary Committee of inquiry, appointed on 10th September, 1974 and reporting to the Parliament on 27th November 1975 had this to say [8],:
’… claims from orthodox physicians that chiropractors had caused gross harm also proved to be elusive. The Committee was often warned in the early months of its inquiry about numbers of chiropractic victims— but as it searched for them they receded into the mists like the Angels of Mons.’
2.3 RISK OF CHIROPRACTIC ADJUSTMENT
Having asserted that the chiropractic profession has been shown to deliver care that has, for the most part, been found to be beneficial and without dangerous side effects it is important that any risk factor be identified, if at all possible through on-going investigation of all practices utilised by this growing profession. Where can such an investigatory body or organisation be found?
2.3.1 THE NATIONALCENTER FOR COMPLEMENTARY AND ALTERNATIVE MEDICINE
In the United States of America, the birthplace of chiropractic, the National Center for Complementary and Alternative Medicine (NCCAM) is the US Federal Government’s lead agency for scientific research on Complementary and Alternative Medicine (CAM). This body is one of the 27 institutes and centers that make up the National Institutes of Health (NIH) within the U.S. Department of Health and Human Services [11].
The NCCAM has a three point Mission:
- Explore complementary and alternative healing practices in the context of rigorous science.
- Train complementary and alternative medicine researchers
- Disseminate authoritative information to the public and professionals.
In carrying out its mission NCCAM has focused on four primary areas:
- The advancement of scientific research: Having funded over 2,500 research projects at scientific institutions across the United States and around the world.
- The training of CAM researchers: Supporting the training of new researchers as well as encouraging experienced researchers to study CAM.
- Sharing news and up to date information: Using all available means through electronic media, fact sheets, lectures, continuing medical education programs and various publications.
Supporting integration of proven CAM therapies. This research is intended to help both the public and health professionals understand which CAM therapies have been proven to be safe and effective.
The research conducted to date by the NCCAM appears to be quite comprehensive but there is more in train. In looking at the consequences of spinal manipulation for low back pain, “Information for Consumers” was encapsulated in the May 2009 Newsletter or Fact Sheet under a section entitled “Get the Facts”.
Some details are presented relating to the frequency of low back pain in the USA and the use of manipulative procedures in caring for such problems, mention is made of ‘Study Findings to Date’ and the challenges facing researchers. Side effects and risks are touched upon and the observation is made that “The rate of serious complications from spinal manipulation, although not definitely known, appears to be very low overall.” Information is then presented about the potential complication from low-back manipulation of cauda equina syndrome but the assurance is given that,” Reports indicate that cauda equina syndrome is an extremely rare complication.” Some mention is made of projects supported by NCCAM in the study of spinal manipulation [12].
See Chapter 7. #24.GertBronfort, DC, PHD Minnesota
#16.William C. Meeker, DC, MPHSan Jose, California
For those interested in gaining more detailed information an expanded version of this ‘fact sheet’ is made available by NCCAM. *This expanded fact sheet includes selected references and additional resources. It is also possible to order a printed version from the NCCAM Clearinghouse.
*URL: nccam.nih.gov/health/pain/spinemanipulation.htm
2.3.2 RISK OF ADJUSTMENT ON CERVICAL/NECK TREATMENT
Klougart, et al conducted a study in Denmark in 1996 and determined that the risk of stroke after cervical spine manipulation was low. They noted that manipulation of the two upper cervical vertebrae into passive rotation showed the greatest risk [13].
Lauretti [14] summarise the studies that have discussed the risk of cervical spine manipulation. Among the findings are that, serious complications arise after manipulation of the cervical spine at a frequency of 1 in 4 million manipulations or fewer. The results of a RAND Corporation review provided an estimate of “one in a million.” A study by Dvorak of 203 manual medicine practitioners in Switzerland, found no deaths reported and a rate of one serious complication per 400,000 cervical manipulations. Jaskoviak’s study from the National College of Chiropractic Clinic in Chicago from 1965-1980 showed no cases of serious injury or vertebral artery stroke. A study of over half a million adjustments at the Canadian Memorial Chiropractic College outpatient clinic over a nine-year period by Henderson and Cassidy also found no serious injuries. [14]
2.3.3 NORMAL ACTIVITIES
“Dr William J Lauretti, a chiropractic researcher from Bethesda, Maryl and spent over 12 years in private practice before joining the Chiropractic Clinical Science faculty at New York Chiropractic College in 2005. He has written numerous journal articles and textbook chapters about the risks of chiropractic neck treatments, and has lectured extensively on the topic. He has been interviewed by major news outlets about chiropractic risks, including CNN, The Boston Globe, The San Francisco Chronicle and Reuters International News Service. Dr. Lauretti has also served as Editorial Director for ‘Chiropractic OnLine’ The American Chiropractic Association’s Web Page” [15].
He has pointed out that there are many different ways to injure the vertebral artery. These are noted in the medical literature and include administering anesthesia during surgery, bending the neck backwards for dental work and when taking X-rays. Furthermore a host of normal activities such as using a telephone, overhead work, and bending the neck over a sink to wash the hair have also been shown as causes of vertebral artery dissection [16].’
2.3.4 RISKS OF OTHER COMMON TREATMENTS FOR NECK SYMPTOMS
In order to gauge the relative risks of chiropractic neck treatment it is informative to compare the risks of associated with other treatments for similar problems. For example, Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) prescription has a 4/10,000 annual mortality rate from drug induced gastrointestinal ulcers among patients treated for musculoskeletal pain. That equates to about 3,200 deaths per year in the US where the study was conducted [14].
Even short term NSAIDs usage has been shown to cause GI complications and can’t be deemed less risky than long term usage. Other procedures such as neck surgery show a 3-4% complication rate and there are about 4,000-10,000 deaths per million neck surgeries [14].’
Extracts taken from:What are the Risk of Chiropractic Neck Treatments? by William J.Lauretti. Available from: URL:http://www.chiro.org/chimages/chiropage/cva-1.html
2.3.5 OTHER STUDIES DISCUSSING RISK OF CHIROPRACTIC ADJUSTMENT ON CERVICAL/NECK TREATMENT
- ‘Stroke After Chiropractic Neck Manipulation a ‘Small but Significant Risk’ says American Heart Association’ [17]
Dissection of the vertebral arteries was the cause of the strokes in this study according to the survey data. A dissection is when the walls of the artery split apart, blood then accumulates and eventually blocks the circulation to the brain.
The studies co-autherDrPhillp Lee noted that most allopathic invertentions had higher complication rates than chiropractic treatments.
Extracts taken from: “Stroke after chiropractic neck manipulation a ‘small but significant risk,” says American Heart Association by Editorial Staff, Dynamic Chiropractic. Available from: URL:http://www.chiroweb.com/mpacms/dc/article.php?id=41126
- Chiropractic Does Not Increase Risk of Stroke
A February 2008 study published in the journal Spine has concluded that there is no support for there being any excess risk of stroke following chiropractic manipulation.In particular the authors noted that patient were just as likely to suffer a stroke after visiting the family doctor as compared to the chiropractor.
The ACA feels that this may be one of the most significant pieces of research in the profession’s history. A similar paper from 2001 published in the Canadian Medical Association Journal found a one-in-5.85-million risk of stroke with a chiropractic neck adjustment. In this their 2008 study, the Canadian team examined nine years of data from Ontario. They found only 818 patients reported a vertebrobasilar artery (VBA) stroke out of a total population of 11.5 million people. The investigators not only studied the relationship between VBA &chiropractic visits, they also examined VBA and family doctor visits.
Thus the researchers were able to state that “Because the association between chiropractic visits and VBA stroke is not greater than the association between PCP visits and VBA stroke, there is no excess risk of VBA stroke from chiropractic care [18].”
Extracts taken from: Chiropractic Safety: Chiropractic Does Not Increase Risk of Stroke. Available from: URL:http://www.drrisley.com/html/chisafe.html
2.3.6 NEW RESEARCH SUPPORTS THE SAFETY OF UPPER CERVICAL ADJUSTMENTS
2.3.6.1 The first paper, from England, was published in Spine 32(21): 2375-2378, October 1, 2007 and its conclusions are thus:[19]
No reports of serious adverse events from over 50000 observed cervical spine manipulations. There were reports of Minor side effects such as dizziness which usually arose immediately or with one week after the manipulation. The rates for Minor side effects are:
- 16 per 1,000 treatments for fainting, dizziness, light-headedness
- 15 per 1,000 treatments for upper limb numbness or tingling
- Four per 100 treatments for headache.[19]
2.3.6.2 The second study was published in Spine (February 2008).Another project, headed by Canadian researchers, found that the risk of a stroke is no different whether people go to a chiropractor or a medical doctor! As a special note, the numbers found in this study support the “one-in-a-million” event rates that chiropractors have always claimed. [20]
The Study reported in the journal ‘Spine’ is identified as follows:-
- Risk of Vertebrobasilar Stroke and Chiropractic Care: Results of a Population-Based Case-Control and Case-Crossover Study [20]
The study was designed to examine for associations between chiropractic visits and vertebrobasilar
artery (VBA) stroke and to compare this with primary care physician (PCP) visits and VBA stroke.
For a case to be included in the study the patient needed to have a VBA stroke and be admitted to an Ontario hospital within the study period of nine years (1993-2002) Health billing records were used to determine whichDoctors a patient had visited.
The data showed there were only 818 VBA strokes hospitalized from a population of greater than 100 million person-years. For patients aged below 45 years, the identified cases were three times more likely to see a chiropractor or a PCP before their stroke than controls.. For cases above 45 years there was no increased association. There were positive associations found between stroke and PCP visits across all age groups. VBA stroke was highly associated with visits for headache and neck complaints based on billing records..
Overall results found that VBA stroke is a very rare event. It was suggested that headache and neck pain resulting from the artery dissection, but preceding a stroke was the cause or an increased risks of VBA stroke associated with chiropractic and PCP visits. There was no evidence identified to suggest any excess risk of VBA stroke when seeking chiropractic care compared to primary care [20].”
Extracts taken from:Risk of Vertebrobasilar Stroke and Chiropractic Care: Results of a Population-Based Case-Control and Case-Crossover Study by Cassidy JD, Boyle E, Côté P, He Y, Hogg-Johnson S, Silver FL,Bondy SJ. Spine 2008 Feb 15;33(4S):S176-S183.
2.3.7 FURTHER MEDLINE ARTICLES ON CHIROPRACTIC SAFETY
- A Risk Assessment of Cervical Manipulation vs. NSAIDs for the Treatment of Neck Pain [21]
This study [21] was a literature review to address the following questions:
- What is the risk of serious injury or death after cervical manipulation?
- What is the evidence that cervical manipulation is a useful treatment for neck pain?
- What are the risks and usefulness of non steroidal anti-inflammatory drugs (NSAIDs) as a treatment for musculoskeletal disorders?
Articles for review were found from 1966-1994 through a literature search with key words such as chiropractic manipulation, non-steroidal anti-inflammatory agents and adverse effects. Only those studies that had a numerical estimate of risk were included. Also included were randomized and controlled studies that of manipulation or NSAID use for neck pain that were focused on effectiveness.
From the literature it was found that there were no RCTs for NSAID use and neck pain. There were a few well conducted trials for manipulation. The study authors were left to conclude that the best evidence suggests that cervical manipulation is much safer for neck pain than using NSAIDs. This could be by a factor of up to several hundred times. They also concluded that there is no evidence to indicate NSAID are more effective for neck pain than cervical manipulation.
Extracts taken from: A Risk Assessment of Cervical Manipulation vs. NSAIDs for the Treatment of Neck Pain byDabbs V, Lauretti WJ. J Manipulative PhysiolTher 1995 Oct; 18(8):530-536.[21]
- Misuse of the Literature by Medical Authors in Discussing Spinal Manipulative Therapy Injury [22]
This study examined the use of the words chiropractic and chiropractor in the published literature, particularly in relation to the documenting of cervical manipulation complications. The study involved the collection of recent published articles about spinal manipulation iatrogenesis. Articles that mentioned either chiropractic and/or chiropractor were examined to determine the actual training of the practitioner involved in the iatrogenic incident. There were three methods used to determine the training of the practitioner, they were (1) writing to the authors of the published studies; (2) reviewing previous publications and (3) reviewing subsequent publications.
The results of this study revealed that “chiropractic” and “chiropractor” often arise in the literature when iatrogenic complications, method of manipulation and manipulation practitioner are reported. Irrespective of the presence or absence of actual chiropractic training.
The author concludes that
“The words chiropractic and chiropractor have been incorrectly used in numerous publications dealing with SMT injury by medical authors, respected medical journals and medical organizations. In many cases, this is not accidental; the authors had access to original reports that identified the practitioner involved as a nonchiropractor. The true incidence of such reporting cannot be determined. Such reporting adversely affects the reader’s opinion of chiropractic and chiropractors” [22].”
Extracts taken from: Misuse of The Literature by Medical Authors in Discussing Spinal Manipulative Therapy Injury by Terrett AG.J Manipulative PhysiolTher 1995 May;18(4):203-210.
- Is Cervical Spinal Manipulation Dangerous? [23]
This report was a case study which sort to address the concerns about cerebrovascular accidents after cervical manipulation.The case documented is of a cerebrovascular infarction without sequelae. The case reports of a 39-year-old man with nonspecific neck pain,treated by a family doctor with cervical manipulation. [23]
Post-manipulation the patient had a severe headache and neurologic symptoms. These symptoms disappeared completely within a period of 3 months. However permanent signs of a cerebellar infarction remained on computed tomography and magnetic resonance imaging. The patient was followed-up after 7-years and it was found that he was working full-time and had no neurologic symptoms. Imaging of the cervical blood vessels showed them to be normal although the MRI still showed signs of left sided infarction.[23]
Extracts taken from: Is cervical spinal manipulation dangerous? by Licht PB, Christensen HW, Hoilund-Carlsen PF. Department of Clinical Physiology and Nuclear Medicine, Odense University Hospital, DK-5000 Odense, Denmark. J Manipulative PhysiolTher. 2003 Jan 26(1):48-52.
- Inappropriate Use of the Title ”Chiropractor” and Term “Chiropractic Manipulation” in the Peer-Reviewed Biomedical Literature [24]
The misuse of the words chiropractor and chiropractic manipulation, in relation to cervical spine manipulation injuries has been discussed earlier [22]. This study sort to–(1) prospectively study the literature for articles that reported an association between injury and chiropractic, or chiropractic manipulation.; 2) Determine the basis for the use of the word chiropractor or chiropractic manipulation by directly contacting the authors of the papers found.; 3) Document the results of submitting letters to the journals where inaccurate reports were contained.
Articles were identified using only the PubMed electronic database for the period from June 2003 to May 2004. Articles identified were reviewed and as needed, the authors were contacted via email to ascertain the qualifications or profession of the manipulation provider. A letter was also sent to the editor of each journal identified.
Twenty four (24) different cases from six publications, were identified. All of the cases occurred one of two European countries. In all the publications the study authors implied that it was a chiropractor and that each patient underwent chiropractic cervical spine manipulation before developing symptoms of injury. Upon contacting the authors, one author conceded that it was not a chiropractor involved. Two authors did not respond. A further author of a case series admitted that the term chiropractor had been misused. Four journals accepted and published letter to editors and one journal published a correction.
The results of this study indicate that European biomedical researchers have misused chiropractic related terms when reporting cervical spine manipulation injuries. It is also worth noting that the inaccurate use of terminology has also gone through a peer-review process without correction.
Extracts taken from: Inappropriate Use of the Title Chiropractor and Term Chiropractic Manipulation in the Peer-Reviewed Literature by Lawrence H.Wyatt. ChiroprOsteopat2006 Aug 22; 14(1):16. [24]
2.3.8 Risk of adjustment on lower back treatment
- Safety of Spinal Manipulation in the Treatment of Lumbar Disk Herniations: a Systematic Review and Risk Assessment [25]
This study was a systematic literature review focused on the risk of spinal manipulation for the treatment of lumbar disk herniation.It also aimed to estimate the risk of spinal manipulation on lumbar disk creating a severe negative reaction.
A literature search was undertaken to identify relevant published literature such as case reports, reviews that documented lumbar disk herniation treatment with spinal manipulation and those that reported adverse events or risks. Once appropriate papers such as prospective and retrospective studies were identified, they were assessed for quality and various results and conclusions were tabulated. The results of the study provide a risk of less than 1 in 3.7 million of spinal manipulation leading to a clinically worsened disk herniation. [25]
Extract taken from: Safety of spinal manipulation in the treatment of lumbar disk herniations: a systematic review and risk assessment by Oliphant D. J Manipulative PhysiolTher. 2004 Mar-Apr;27(3):197-210. [25]
References
- Chiropractic effects on athletic ability.Lauro A. Mouch B.Chiropractic:The Journal of Chiropractic Research and Clinical Investigation. 1991; 6:84-87 Available from URL: http://www.kimfamilychiropractic.com/sports.html
- WFC Quarterly World Report. President’s message. 2010 Mar 31. 1-2.
- Leboeuf-Yde C, Axén I, Ahledeldt G, Lidefelt P, Rosenbaum A, Thurnherr T. The types and frequencies of improved nonmuskuloskeletal symptoms reported after chiropractic spinal manipulative therapy. J Manipulative PhysiolTher 1999;22 (9):559–564. Available from URL: http://www.cascadewellnessclinic.com/benefits.shtml
- Manga P. Angus D. Papadopoulos C. Swan W. The effectiveness and cost- effectiveness of chiropractic management of low-back pain. Richmond Hill, Ontario: Kenilworth Publishing, 1993.p.79, 11, 13.
- National Library of Medicine. 14: Acute low back problems in adults clinical practice guideline: AHCPR Publication No. 95-0642 [Online]. 1994 Dec [cited 2010 Mar]; Available from:URL:http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=hsarchive&part=A25870#top
- US Department of Health and Human Services. New federal study recommends spinal manipulation for back pain relief, Dallas: PR Newswire [Online]. 1994 Dec 8 [cited 2010 Mar]; Available from: URL:http://www.silcom.com/~dwsmith/qcover.html
- Chiropractic in New Zealand report. New Zealand: Government Printer Wellington; 1979.p.206-207, 77-78.
- Victoria Parliament: Joint Select Committee on Osteopathy, Chiropractic and Naturopathy. Report from the osteopathy, chiropractic and naturopathy committee. 1975 Nov 27, p.17, para 4,3,10.
- Bigos SJ, Richard Bowyer RO, Braen RG, Brown K, Deyo R, Haldeman S, Hart JL. Acute low back problems in adults: clinical practice guidelines. Agency for Health Care Policy and Research Publication No. 95-0642 – U.S. Department of Health and Human Services; 1994 Dec.
- Hasselberg PD. Commision of inquiry into chiropractic. Wellington (NZ): Government Printer Wellington, 1979.
- NCCAM Facts-at-a-Glance and Mission. National Center for Complementary and Alternative Medicine [Online]. 2010 [cited 2010 Mar]; Available from: URL:http://nccam.nih.gov/about/ataglance/
- National Center for Complementary and Alternative Medicine. Get the facts: spinal manipulation for low-back pain [Online]. 2009 May [cited 2010 Mar]; Available from: URL: http://nccam.nih.gov/health/pain/spinemanipulation.htm
- Klougart N, Leboeuf-Yde C, Rasmussen L. Safety in chiropractic practice: part I: the occurrence of cerebrovascular accidents after manipulation to the neck in Denmark from 1978-1988. J Manipulative PhysiolTher 1996;19(6):371–377. Available from: URL http://www.ncbi.nlm.nih.gov/pubmed/8864967
- Lauretti W. What are the risk of chiropractic neck treatments? [Online]. [cited 2010 Mar]; Available from: URL:http://www.chiro.org/chimages/chiropage/cva-1.html
- Media Spokesperson Biographies. American Chiropractic Association. [online] [cited 2012 Apr]; Available from: URL: http://www.acatoday.org/content_css.cfm?CID=2163
- Lauretti W. What are the risk of chiropractic neck treatments? [Online].[cited 2012 Apr];Available from: URL: http://www.acatoday.org/pdf/chiro-risks.pdf
- Editorial Staff. “Stroke after chiropractic neck manipulation a ‘small but significant risk,” says American Heart Association. Dynamic Chiropractic [Serial online] 1994 Mar 11 [cited 2010 Mar];12,(6). Available from: URL:http://www.chiroweb.com/mpacms/dc/article.php?id=41126
- Chiropractic Safety. Chiropractic does not increase risk of stroke [Online] [cited 2010 Mar]; Available from; URL:http://www.drrisley.com/html/chisafe.html
- Silk S. Death of the dogma of critical injury: new research lays ‘the great stroke Hoax’ to rest. Canadian Chiropractor [Online]. 2007 Dec [cited 2010 Mar]; Available from: URL:http://www.canadianchiropractor.ca/content/view/830/67/
- Cassidy JD. Boyle E. Côté P. He Y. Hogg-Johnson,S. Silver FL, et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study spine. Spine [Serial online] 2008 15 Feb [cited 2010 Mar];33(4S):S176-S183. Available from: URL:http://journals.lww.com/spinejournal/Abstract/2008/02151/Risk_of_Vertebrobasilar_Stroke_and_Chiropractic.19.aspx
- Dabbs V, Lauretti WJ. A risk assessment of cervical manipulation vs. NSAIDs for the treatment of neck pain. J Manipulative PhysiolTher 1995 Oct;18(8):530-536. Available from URL: http://www.ncbi.nlm.nih.gov/pubmed/8583176
- Terrett AGJ. Misuse of the literature by medical authors in discussing spinal manipulative therapy injury. J Manipulative PhysiolTher 1995 May;18(4):203-210.Available from URL: http://www.ncbi.nlm.nih.gov/pubmed/7636409
- Licht PB, Christensen HW, Hoilund-Carlsen PF.Is cervical spinal manipulation dangerous?.J Manipulative PhysiolTher [Serial online] 2003 Jan [cited 2010 Mar]; 26(1):48-52. Available from: URL:http://www.ncbi.nlm.nih.gov/pubmed/12532139
- Wyatt L. Inappropriate use of the title chiropractor and term chiropractic manipulation in the peer-reviewed literature. ChiroprOsteopat2006 Aug 22;14(1):16. Available from: URL: http://www.ncbi.nlm.nih.gov/pubmed/16925822
- Oliphant D. Safety of spinal manipulation in the treatment of lumbar disk herniations: a systematic review and risk assessment. J Manipulative PhysiolTher. 2004 Mar-Apr;27(3):197-210. Available from: URL: http://www.ncbi.nlm.nih.gov/pubmed/15129202